Arthrofibrosis
Arthro = joint
fibrosis = excessive scarring
On this page
Arthrofibrosis
Arthro = joint
fibrosis = excessive scarring
Introduction
Page navigation hints
If you hover your mouse over the bold, red, lowercase words, a window with more detailed information will pop up. The non-bold, non-underlined, red, lowercase words are hyperlinks that will lead you to more detailed information.
Guiding Principle:
Your clinicians are your teammates. Teammates don’t give up on each other when things get tough; they work together to succeed. I have always understood that Drs. Steadman and Singleton would never give up on me as long as I didn’t give up on myself. You want need to be able to say that about your doctor.
Trauma/Symptoms
- Arthrofibrosis is a rare complication that happens when excessive scar tissue forms in a joint following trauma that involves bleeding (e.g. – knee fracture, infection following routine surgery, knee replacement, or a ligament tear). While it can occur in other joints (shoulders and elbows, for instance), for our discussion, I’m going to stick with knees.
- Arthrofibrosis results in any or all of the following:
- stiffness and pain
- inability to fully bend (flexion) the knee
- inability to fully straighten (extension) the knee
- patellar (kneecap) immobility
- heat – either locally or generally over the entire knee
- Every case of arthrofibrosis is different. Some people present with pain, stiffness, patellar immobility, and are lacking only extension (that was my case), whereas others may only lack flexion, or have another combination of symptoms.
- If you have any of these symptoms following trauma, please take them seriously and see a doctor, but not just any doctor. Below, I’ll talk about how to choose one.
- Following surgery or other trauma, you may initially feel like you’re healing. However, as you start to load your joint more (weaning off crutches, walking, standing), you may begin experiencing disproportionate pain and stiffness (especially in the front of your knee) along with an inability to bend and/or straighten your leg. It’s worth mentioning again that arthrofibrosis is rare, but the sooner it can be addressed, the better the outcome.
Choosing a medical team
- I cannot overstate the importance of choosing a proper care team. Since arthrofibrosis is rare, few doctors specialize in treating it.
- Remember: Seeing the wrong doctor saves you neither time nor money. There’s a good chance the “best” in your hometown has rarely seen arthrofibrosis. Such was the case with me. There’s also a good chance you’ll need to travel to see an expert.
- You need a doctor and physical therapist experienced with arthrofibrosis.
- It has been my (and my clients’) experience that few orthopedic doctors have the innate patience to elegantly manage a chronic condition. By elegant I’m referring to management of the emotional and surgical complexities of a chronic condition.
Too often my clients have worked with a doctor who “cleans out scar tissue.” I lived this scenario twice. It’s important to talk with your doctor about their methods of “cleaning out scar tissue,” and what tools they’re using.
Your clinicians are your teammates. Teammates don’t give up on each other when things get tough; they work together to succeed. I have always understood that Drs. Steadman and Singleton would never give up on me as long as I didn’t give up on myself. You want need to be able to say that about your doctor.
Since every case is different–from symptoms to surgery to rehabilitation–you need a physical therapist familiar with arthrofibrosis’s variability as well as scar physiology. Your medical team’s understanding that scar grows in response to load is key to your rehabilitation.
Diagnosis
- Getting a proper diagnosis is your foundation but can be a torturous journey for many. Finding a doctor who is intimately familiar with arthrofibrosis will save untold suffering.
- Be aware that sometimes scarring does not show up well on MRI or isn’t appreciated by a radiologist not specifically looking for it. This happened to me at my local imaging center, even though I had significant arthrofibrosis.
- Arthrofibrosis can be seen most clearly on an image produced by a 3 Tesla MRI. At The Steadman Clinic, imaging equipment can be set to produce the best image of the scarring possible; also, the radiologists are experienced at reading images of knees with arthrofibrosis. If you can’t get to the Steadman Clinic, ask your doctor and radiologist straightforward questions about their experience diagnosing arthrofibrosis. If you don’t receive a clear and convincing answer, get a second (or third) opinion. Multiple opinions are easier than multiple surgeries.
- Observe: A doctor experienced with arthrofibrosis will use their hands to feel the temperature of your knee (often knees with arthrofibrosis will feel hot, and they may not have much, if any, swelling) and restriction with popping/grinding as you bend and straighten. Fancy equipment will get you a nice image, but your trust is best placed in a good set of hands.
Treatment
Arthroscopic surgery [on a knee with arthrofibrosis] can be complex and technically challenging; therefore, choose a doctor who has both significant arthrofibrosis experience and advanced surgical skills–the scarring associated with arthrofibrosis changes the way your knee looks through a scope, including altered tissue planes that can distort normal anatomy.
Treatment the wrong way
- Too often my clients have worked with a doctor who “cleans out scar tissue.” I lived this scenario twice. It’s important to talk with your doctor about their methods of “cleaning out scar tissue,” and what tools they’re using.
- Why do tools matter? Most of my clients with arthrofibrosis, myself included, have had failed surgeries during which scar tissue was “cleaned out” using a tool called a shaver (also called a debrider).

Shaver 1
View 1 of shaver

Shaver 2
View 2 of shaver
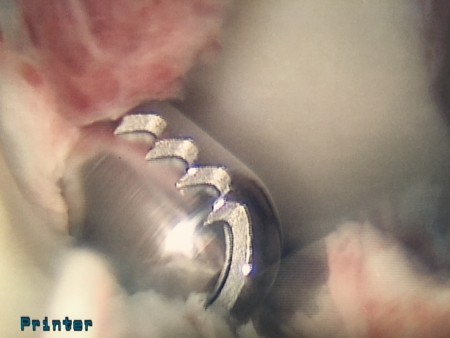
Shaver 3
View 3 of a shaver
- While this is an important arthroscopic tool, it is not well suited to address arthrofibrosis. It isn’t precise, and by virtue of shredding scar tissue, it causes bleeding–sometimes profuse bleeding. My two pre-Steadman Clinic surgeries required use of a tourniquet to stop bleeding. Earlier, I mentioned bleeding can lead to scar tissue formation, so by using a shaver/debrider, the very environment that resulted in scarring to begin with is recreated.
- If you’ve had a previous failed surgery, have a look at your surgical images and see if you notice a shaver in the photo.
Treatment the right way
According to Dr. Steadman, there are three main components to arthrofibrosis (while everyone shares number 1, not everyone will have numbers 2 and 3), each of which is treated with different modalities.
1) Scar
Surgery addresses the scar as well as any pain-producing areas inside the joint. An anterior interval release can be accompanied by synovectomy (an arthroscopic procedure to remove inflamed synovial tissue) and chondroplasty.
- Drs. Steadman and Singleton strive for a “bloodless surgery.” Tourniquets are not used in the operating room during arthrofibrosis surgeries because they are not necessary.
- The goal of surgery is to release scar tissue causing restriction. It’s likely that not all of your scarring is symptomatic. Drs. Steadman and Singleton determine, based on history, physical exam, and imaging which scarring is causing restriction and a meaningful loss of space within the joint. Cleaning out every ounce of scar tissue is not the focus (see my first point under “treatment the wrong way”).
- Dr. Steadman found using a heat probe called an ArthroCare Wand allowed him to precisely address offending scar tissue by burning and releasing it. (Pardon the notes on the images.)

ArthroCare Wand
ArthroCare Wand

ArthroCare Wand pre-release
Using the ArthroCare Wand (pre-release)

ArthroCare Wand during release
Using the ArthroCare Wand (during release)

Arthrocare Wand after release
Using the Arthrocare Wand (after release)
- Arthrofibrosis surgery is the intersection of medicine and art. Your doctor needs to have the experience to carefully and gently identify aberrant scar, address it, and leave non-symptomatic scar alone.
- Drs. Steadman and Singleton finish each surgery by slowly decreasing the saline pump pressure, thereby decreasing the pressure inside the knee joint, and looking for bleeding. Using the ArthroCare Wand allows them to cauterize any bleeding before the knee is closed.
2) Joint capsule tightness
Here’s some terminology and a diagram to help navigate the knee from the outside in.
- The joint capsule is soft tissue containing the synovium and synovial fluid.
- Synovium is the lining on the inside of the capsule that makes synovial fluid.
- Synovial fluid lubricates the joint and acts as a secondary shock absorber to the cartilage.

- Scarring results in a loss of range of motion that can result in joint capsule tightness.
- Improper functioning caused by joint capsule tightness may increase wear and tear on cartilage and other joint structures.
- In some cases, after the scarring has been ameliorated through surgery, joint capsule tightness will also need to be addressed.
- Insufflation addresses joint capsule tightness.
- Insufflation is a fast and effective procedure performed under general anesthesia. Approximately 100mL (the actual amount varies for every individual and is usually between 60 and 180mL) of saline is introduced into the joint capsule causing it to stretch, increasing space inside the joint. After several minutes (variable from 30-60 seconds up to 5 minutes), the saline is removed and you’ll be on your way to recovery.
- I required surgery (anterior interval release/synovectomy/chondroplasty) plus two insufflations before regaining my full range of motion.
- Please note that while the insufflation procedure is relatively straightforward, it is a further insult to an arthrofibrotic knee and, in my experience, post-op recovery and rehabilitation was very nearly as slow and methodical as after my arthroscopic surgeries.
3) Inflammation
- Have you noticed that your knee feels warm? That’s inflammation.
- Inflammation is part of arthrofibrosis, and, left unchecked, results in more scarring.
- Steroid injections and pills may address inflammation. Ice helps too. I’ve logged thousands of hours attached to my ice machine. When ice failed, steroid injections and pills have helped.
Physical therapy
- With arthrofibrosis, the best surgical outcome can be ruined by an inappropriate physical therapy regime.
- Your physical therapy should never be rough and forceful.
- In my experience, extreme diligence and restraint over an extended period (many months) is paramount. Remember that friend with a muscle tear, or whatever, who pushed through it and eventually got better anyway, even while ignoring most of her physical therapy exercises? Arthrofibrosis is not nearly so forgiving. Promise me that you won’t push your luck.
- With the consent of your physical therapist, back off on your activities–immediately–any time you feel increased heat, tightness, or pain.
- Learn to love your CPM (Continuous Passive Motion) and ice machines.
- Ice frequently, but avoid frostbite, which has the alarming effect of increasing heat in the area you are trying to cool while precluding further icing until it recovers. Always place a towel between your ice and skin.
- Take a page out of the cyclist’s bible: don’t stand when you can sit and don’t sit when you can lie down.
- My post-operative physical therapy regime included a lot of patellar mobilizations, extension mobilizations, gentle range of motion exercises, and quadriceps control exercises. Understand that re-mastering movement patterns will require thousands of tedious exercise repetitions that serve as your foundation for rebuilding. Embrace wall slides, or whatever your least favorite mind-numbing exercise may be. Be persistent.
Arthrofibrosis surgery is the intersection of medicine and art. Your doctor needs to have the experience to carefully and gently identify aberrant scar, address it, and leave non-symptomatic scar alone.
Expectations
- I’m aware that what I’m about to share may evoke nightmares of arthrofibrosis prison. There’s good news. If you have proper expectations, you’re more likely to have a positive outcome. The following is based on my experience. Since every case is different, your experience will be different, but I do know my experience is similar to that of many arthrofibrosis patients I’ve met and clients with whom I’ve worked.
- Fresh out of surgery–and sometimes for months–simply sitting in a chair with your knee below your heart may cause it to get hot. It seems ridiculous, but it’s true. It took me 7 months after my first surgery with Dr. Steadman to be able to sit in a chair for an hour without my knee getting fiery hot. Remember, heat promotes regrowth of the scar; it’s very important to keep heat and inflammation to a minimum.
- Progress will be–and has to be–glacially slow. It took me almost a year to do a straight leg lift with control over my lower leg.
- Nobody will be able to tell you how many surgeries you’ll need and when you will be better, or to what extent you’ll improve. That’s because all cases are different (I sound like a broken record, I know.). At some point, you’ll have to make peace with the indefinite. Wake up every day and do your therapy with the recognition that big gains come from an accumulation of small gains.
- The grocery story will become Mt. Everest. Get help with shopping and cooking.
- Other people you meet at physical therapy with seemingly worse injuries will get better faster than you. Don’t compare your journey to theirs. Arthrofibrosis is chronic.
- It’s highly unlikely that your affected side will ever feel like your unaffected side. In most cases, that doesn’t mean you can’t eventually have a functional leg.
- You will grow weary of moving your kneecap back and forth. Don’t overlook seemingly simple exercises.
- You’re going to need a lot of help, especially for the first 3 months after surgery.
- Learn to embrace being on your back. You’re likely to spend many hours each day (sometimes for weeks or months) in a CPM. Think of it as training for a gold medal in the sofa surfing Olympics.
- Since you won’t be able to move like you’re accustomed to, work with your physical therapist to create an aerobic training program that’s injury friendly (think hand bike, one-legged rowing machine, or swimming with a pull buoy). Also, ask for a few good core drills. You wouldn’t believe how much training it takes to lie down for 6 hours a day strapped to a machine that’s slowly bending and straightening your knee. If you don’t train your core, your back will revolt.
- I purchased this machine at The Steadman Clinic. It has served me well for three years and is still going strong. Setting it up on a chair so the pump doesn’t have to work too hard will keep it quiet.
- These crutches (covered by most insurance) win the most improved gimp paraphernalia award. Get crutch crampons if you live in a snowy climate.
- Find yourself a hobby that is gimp-friendly. For some ideas, click here.
Inspiration
I know this is all overwhelming. I’ve been where you are. Please know you aren’t alone, and that with dedication and patience, it does get better. People with arthrofibrosis–me included–do recover and can regain the strength to connect with old activities. Hopefully now you feel empowered to take the next steps on your journey.
Arthrofibrosis Recovery Guide
My clients’ victories, questions, anxieties, and resilience led me to record what I’ve learned about arthrofibrosis recovery in plain English.
My hope is that this booklet will leave you feeling empowered and informed. You aren’t alone. I’ve been where you are right now and have helped others in your position. It gets better. Follow the guidance in this booklet.
I’d like to thank Dr. Singleton for fact-checking and providing feedback on this booklet.
Arthrofibrosis Guide under maintenance
Thank you to Dr. Sheila Strover for this brilliant educational video about arthrofibrosis.
READ NEXT
My arthrofibrosis success story
Arthrofibrosis is one of the most challenging orthopedic conditions to treat and manage--for a lifetime. It impacts far more than a joint. It can affect mental health, finances, careers, and relationships. My own journey began in 2010 with a severe knee fracture, eight surgeries, and more than four years on crutches.
1-on-1 coaching
You don’t have to recover alone.
Find the right healthcare team | Navigate insurance | Find activities that feel as good at your sport | Talk to another injured athlete who gets it